Methylated vitamins, particularly methyl B12 (methylcobalamin), are active forms of B vitamins that support methylation, a crucial biochemical process involved in DNA repair, gene expression, detoxification, and neurotransmitter metabolism.
However, certain individuals (often many on the autism spectrum) may experience adverse effects due to genetic, metabolic, or health factors.
Below, we outline who should avoid or be cautious with methylated B vitamins, focusing on catechol-O-methyltransferase (COMT) gene variants, methylenetetrahydrofolate reductase (MTHFR) gene variants and other relevant considerations.
1. Individuals with COMT Gene Variants (Slow COMT)
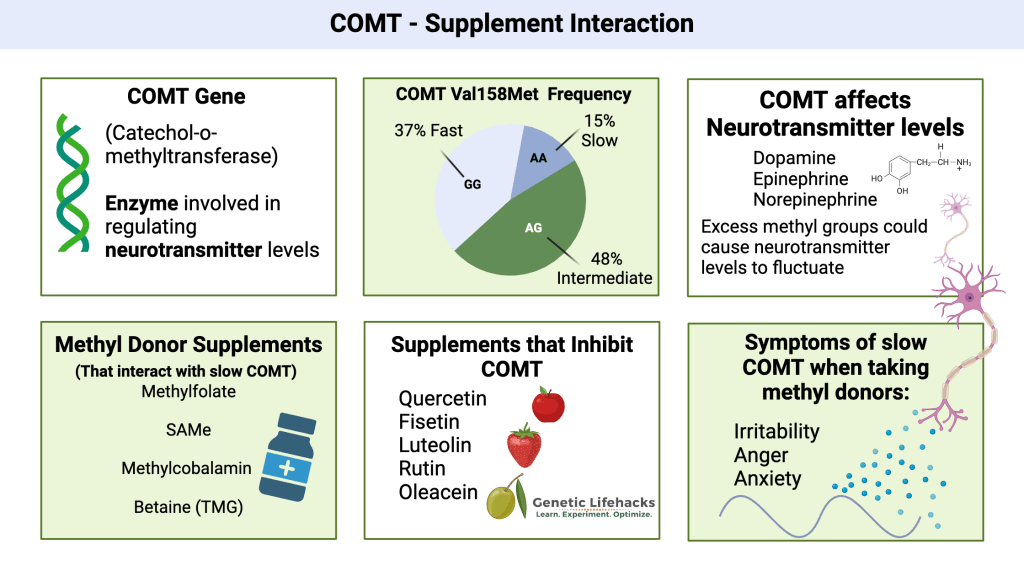
- What is COMT? The COMT gene encodes an enzyme that breaks down catecholamines (dopamine, epinephrine, norepinephrine) by adding a methyl group, a process reliant on methylation.
- Variants in the COMT gene, such as Val158Met (rs4680), can result in “slow” or “fast” COMT activity.
- People with slow COMT (homozygous Met/Met) have reduced enzyme activity, leading to slower breakdown of catecholamines.
- Taking methylated vitamins can increase methylation, potentially causing an excess of dopamine or norepinephrine.
- This may lead to symptoms like anxiety, irritability, agitation, insomnia, or mood swings.
- Recommendation: Those with slow COMT may tolerate non-methylated forms better.
- Alternatives to methyl B12
- Hydroxocobalamin: supports detoxification and is less likely to overstimulate methylation.
- Adenosylcobalamin: Supports mitochondrial energy production and may be better for those with MTR/MTRR mutations or chronic fatigue.
- Best Alternative to 5-MTHF
- Folinic Acid
A non-methylated form of folate that supports folate metabolism without directly contributing to methylation.- Often better tolerated by those sensitive to methyl donors.
- Commonly used in protocols for individuals with methylation issues or autism spectrum disorders.
- Typical dose: 400–800 mcg, Seeking health offers some good options
- Folinic Acid
2. Individuals with MTHFR Gene Variants
- What is MTHFR?
- The MTHFR gene produces an enzyme that converts folate into its active form, 5-methyltetrahydrofolate (5-MTHF), which is essential for methylation and works synergistically with B12.
- Common variants like C677T or A1298C can reduce MTHFR enzyme activity, impairing folate metabolism and potentially leading to high homocysteine levels or B12 deficiencies.
- The MTHFR gene produces an enzyme that converts folate into its active form, 5-methyltetrahydrofolate (5-MTHF), which is essential for methylation and works synergistically with B12.
- Why Be Cautious?
- Some individuals with MTHFR mutations (especially when combined with COMT variants) may be sensitive to methylated supplements. This can occur due to:
- Methylfolate Trap: If B12 is deficient or not properly utilized, supplemental methylfolate (often paired with methyl B12) can accumulate, causing a “methylfolate trap.” This may lead to symptoms like anxiety, fatigue, or neurological issues.
- Overmethylation: Excessive methyl donors (methyl B12, methylfolate) can overwhelm the methylation cycle, particularly in those with impaired methylation pathways, causing side effects like nervousness, rapid heartbeat, or irritability.
- Some individuals with MTHFR mutations (especially when combined with COMT variants) may be sensitive to methylated supplements. This can occur due to:
- Recommendation:
- Start with low doses of methyl B12 or use hydroxocobalamin to avoid overwhelming the system.
- Ensure adequate folate and B6 levels, and address any underlying B12 deficiency before adding methylfolate.
- Genetic testing can clarify MTHFR status.
3. Individuals with Sensitivities to Methyl Donors
- Some people, regardless of genetic status, are sensitive to methylated nutrients (methyl B12, methylfolate, SAMe, TMG).
- Symptoms of sensitivity include anxiety, rapid heartbeat, jitteriness, or insomnia, possibly due to overmethylation or imbalances in neurotransmitter levels.
- Why Avoid?
- Methyl B12 donates methyl groups to the methylation cycle, which can increase SAMe production and affect neurotransmitter balance.
- In sensitive individuals, this may lead to overstimulation or exacerbate existing mental health conditions.
- Recommendation:
- Opt for non-methylated B12 forms (e.g., hydroxocobalamin or adenosylcobalamin) or start with very low doses of methyl B12 under medical supervision.
- Monitor symptoms and consider niacin (niacinimide) to “soak up” excess methyl groups if overmethylation occurs.
4. People with Certain Health Conditions
- Cancer: Some research suggests that high doses of folate and B12 may promote cancer cell proliferation in individuals with existing cancers, as these vitamins support DNA synthesis.
- While evidence is mixed, those with a cancer diagnosis should avoid methyl B12 unless prescribed by a healthcare provider.
- Kidney Issues: High doses of cyanocobalamin (a synthetic B12 form) may impair kidney function in those with borderline kidney problems. While methyl B12 is generally safer, individuals with kidney disease should consult a doctor before supplementing.
- Allergies to Cobalt or B12: Methylcobalamin contains cobalt, and those with cobalt allergies or hypersensitivity to B12 should avoid it.
- Bipolar Disorder or Severe Anxiety: Individuals with bipolar disorder or severe anxiety, especially those with COMT mutations, may experience worsened symptoms due to methyl B12’s impact on dopamine and norepinephrine levels.
5. Other Genetic Variants
- MTR/MTRR Mutations: These genes affect B12 metabolism.
- Individuals with MTR or MTRR mutations may have trouble utilizing B12, leading to deficiencies or poor response to methyl B12.
- They may require higher doses or alternative forms like adenosylcobalamin.
- Individuals with MTR or MTRR mutations may have trouble utilizing B12, leading to deficiencies or poor response to methyl B12.
- VDR Taq Variants: Variants in the vitamin D receptor (VDR) gene, particularly when combined with COMT mutations, can influence dopamine production and B12 tolerance.
- Those with specific VDR Taq and COMT combinations may do better with hydroxocobalamin.
6. Medication Interactions for MB12
- Methyl B12 may interact with certain medications, reducing its absorption or efficacy:
- Metformin: Used for diabetes, metformin can lower B12 levels, and supplemental methyl B12 may not be absorbed effectively.
- Proton Pump Inhibitors (PPIs) or H2 Blockers: These reduce stomach acid, impairing B12 absorption from food or supplements.
- Heavy Alcohol Use: Excessive alcohol consumption can hinder methyl B12 absorption.
- Discuss methyl B12 use with a healthcare provider if taking these medications or consuming significant alcohol.
Genetic Testing:
- If you suspect COMT, MTHFR, or other genetic variants, consider testing (e.g., 23andMe or clinical panels) to guide supplement choices. Work with a functional medicine practitioner to interpret results.
- Start Low, Go Slow: If trying methyl B12, begin with a low dose (e.g., 500 mcg) and monitor for side effects like anxiety, irritability, or insomnia.
- Monitor Biomarkers: Check homocysteine, methylmalonic acid (MMA), and B12 levels to assess methylation status and B12 deficiency.
- Optimal homocysteine is 7–8 µmol/L, and serum B12 should be 500–800 pg/mL.
In summary
The primary groups who should avoid or be cautious with methylated vitamins include:
- Individuals with slow COMT variants
- MTHFR mutations (especially with methyl sensitivity)
- certain health conditions (e.g., cancer, kidney issues)