To be used only if someone requests information on ACC / oral low dose chelation
While this is the ONLY type of chelation we discuss, we are no longer suggesting any type of chelation as a starting point.
The gains it brought were simply not worth the time or utter exhaustion.
We now have more efficient ways (such as peptides) to support the body and help detox happen naturally.
This is not to say that there is no one who needs chelation, but not all children need it and it should not be as broadly recommended as it was in the past.
Below is content written in 2011, it does not reflect my current stance – for reference only:
Taken from: https://www.regardingcaroline.com/andycutler2.html
I’m often asked how people can learn about and begin Andy Cutler Chelation (ACC). Part of the reason for the inquiries is the lack of readily accessible information. When you’re on the outside, it can seem like a secret society, complete with a steep learning curve. However, once you’re indoctrinated, you realize it’s not nearly as difficult as you expected.
The parent network
It’s not for lack of people using Dr Cutler’s protocol that there’s minimal information,
because many thousands of parents use it for their children. It’s safe, inexpensive,
and can be done without a doctor. Could that be why it’s often unknown? There’s
certainly no money to be made from it.
Which means, it’s generally only through parent networks that you’ll learn about
people’s experiences with it. And parents in the thick of recovering a child
sometimes don’t have time to teach others.
THE FAQ’s
Why should I consider chelation?
In 2011, Almost every parent I know who’s tried it says it’s the one thing that truly lifted the veil that separated their
child’s world from their own. Andy has estimated that 75% of children respond.
The reason removing metals can be critical to recovery is because metals impair the
immune system and cause autoimmune disorders.
If your child regressed following vaccines containing mercury, chelation is the
way to remove it.
Keep in mind, chelation can also help with more than just autism. Many parents who
are chelating an ASD child, often chelate their other children with autoimmune
disorders, such as allergies, asthma, PANDAS etc… They repeatedly find their other
children also improve with chelation.
Who was Andy Cutler?
Andrew Hall Cutler, PhD, was a chemist with a degree from Princeton. When his
amalgam fillings gave him mercury poisoning and no one else could help, he
recovered himself using the chelation protocol he developed.
How did he develop his protocol?
Having a background in chemistry, Dr. Cutler knew the importance of half lives. A
half life is the period of time it takes for the amount of a substance be reduced by
half. For example if you take 10 mg of a supplement and it’s half life is 3 hours. In 3 hours you have 5 mg left in your body.
When you take a chelating agent, it binds to metals in your body and escorts them
out. However, every time you stop taking it, the metals it was binding (that haven’t
yet exited) are released into your body. The mobilized metals may be redeposited
into the brain, potentially causing more problems than never chelating in the first
place.
Therefore, Dr. Cutler’s protocol involves frequent, low doses of chelators to keep
them at a fairly consistent level in the blood. Subsequent doses are be given before the prior one releases the metals it was binding, eliminating the danger of
redistribution following each dose.
Using other protocols with higher doses (pulling more than the body can excrete)
and / or infrequent doses (not based half life) is likely to result in pulling mercury
from various areas of the body and releasing it into the brain. A very scary thought.
What chelators are used?
The chelators used in Dr Cutler’s protocol are ALA, DMSA and sometimes DMPS.
ALA (Alpha Lipoic Acid – an antioxidant)
Removes mercury & arsenic from the brain
Does not remove lead
Available over the counter
Must be given every 3 hours (may stretch to 4 hours overnight)
Not to be used by anyone with mercury exposure in the past 3 months
(including people who have received a flu shot, people who have been
exposed to a broken CFL bulb or have amalgam fillings.)
Causes adrenal fatigue (more when used alone)
DMSA (Meso-2,3-dimercaptosuccinic acid)
Removes lead and mercury from organs other than the brain
Does not cross the blood brain barrier.
Available over the counter
Must be given every 4 hours (optionally can give every 3 hrs with ALA)
Known to cause more yeast issues than ALA alone & harder on organs
Used with ALA, speeds the excretion of metals
Lowers neutrophils – resulting in decreased immune function – not
recommended for children with autoimmune issues including PANS/PANDAS
Can use within 4 days of mercury exposure
DMPS (2,3-Dimercapto-1-propanesulfonic acid)
Removes mercury & arsenic, not as good for Lead and not from the brain
Does not cross the blood brain barrier
Transdermal is only available with a prescription
Must be given every 8 hours (optionally ok to give with every other ALA dose)
Used with ALA, speeds the excretion of metals
Not known to lower neutrophils
What is a “Round?”
The chelator(s) you select are administered for 72 hours around the clock; according
to their half life. The 72 hour period is called a “round.” Following a round, you take at least an equal amount of time off and then repeat.
For example, people typically follow a 3 day on / 4 day off schedule, starting on
Friday and continuing through Monday morning. The balance of the week there is
no chelation.
If your child is in school, you should determine the specific hours
which will maximize the time you can chelate.
Rounds can be longer than 3 days, but you should take an equal amount of time off
round as you spent on… so a 5 day round requires a 5 day break. Longer rounds
tend to be harder on the adrenals, so watch for signs of adrenal fatigue. Here are ideas to support https://recoveringkids.com/detox
It’s been estimated that a child with ASD needs between 100 and 300 rounds. I don’t think that many are required.
GETTING STARTED…
Deciding what chelator to begin with:
Often people do several rounds with DMSA initially, to lower the total body burden,
and then add ALA. At least one round this way is recommended.
In our case, we did 2 rounds with DMPS and then added ALA, using them both
together for 32 rounds. Then we switched to DMSA to remove lead, but the lowering
of neutrophils was hard on her. Most of our rounds have been ALA only.
Determining the dose:
Begin with 1/8 mg/lb or less. For future, gradual increases, you may consider
increasing the dose by no more than half of your current dose. You should not
change the dose in the middle of a round. Max dosage is 1/2 mg/lb.
With Caroline, we began with 1/12th mg/lb which was 3mg. Even after 42 rounds,
she is still only at 5mg.
Purchasing the Chelator:
ALA can be bought on amazon or at a health food store. Do not use R-ALA, only
ALA. The main issue is finding capsules small enough to divide into the dose you
need. At a traditional store 100-200 mg capsules will be the smallest you’ll find.
Kirkman Labs sells 25 and 50 mg capsules. The 25 mg also comes flavored if you prefer. Caroline does not mind the unflavored.
Pure encapsulations sells 100 mg (on amazon) which can be ideal if you’re dividing it at home. See our HOW TO MAKE CAPSULES blog for help.
DMSA & DMPS (and also ALA) are available at LIVING SUPPLEMENTS
You can also have DMPS compounded capsules or transdermal with a prescription.
Dividing the Chelator:
If your dose doesn’t match the capsule size you have, you’ll have to divide them into
proper dosages. But don’t despair, it’s not as daunting as it may seem!
I’ve read several methods for how people divide them, but the way I do it is the
easiest for me. Get creative with devising a method that’s best for you!
I use two pill boxes and put the chelator into compartments. See photos at right
Caroline’s dose is 5 mg, and I use a 50 mg capsule (because I want to give her as
little filler as possible at night time).
To Administer the dose, I use a miniature oral syringe, see #3 at right for details.
Insuring you don’t miss a dose:
The timer on your phone can be used, but needing to keep setting it with each dose
is not ideal. I recommend a recurring interval timer app you can set for an interval (such as every 3 hours) and when it beeps, you simply click to advance to the next interval.
You can also set any interval, so if you need to do 2 hr 45 min all day to move up the
bedtime doses, you can. this:
Making a schedule:
Planning out your schedule is important for two reasons:
1. You want to time the nighttime dose so you won’t need to wake up more than once.
2. If you stretch the nighttime dose of ALA to 4 hours, your following day’s times will
need to be adjusted to get the night doses back on track.
For example, here is our typical schedule with ALA every 3 hours (3hr 45min at night)
Day 1
8:30 am / 11:30 am / 2:30 pm / 5:30 pm /. 8:30 pm / 11:30 pm // 3:15 am
Day 2
7:00 am / 9:45 am / 12:30 pm / 3:15 pm / 6:00 pm / 8:45 pm / 11:30 pm // 3:15am
Day 3
7:00 am / 9:45 am / 12:30 pm / 3:15 pm / 6:00 pm / 8:45 pm / 11:30 pm // ….
Notice on days 2 & 3, the daytime doses are shortened to 2h 45 min to ensure that
the nighttime doses don’t get too late, causing multiple night awakenings.
Required Supplements:
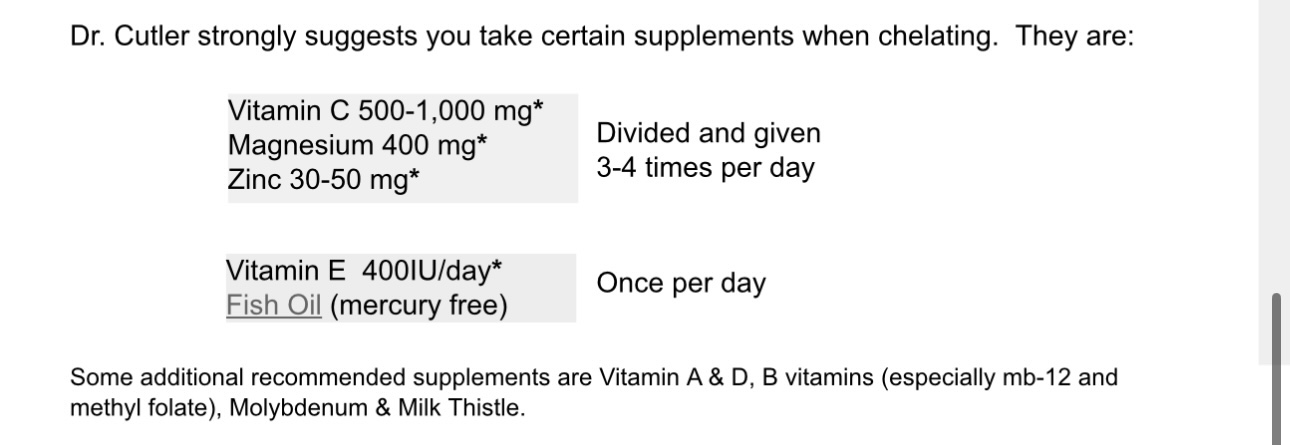
Dr. Cutler strongly suggests you take certain supplements when chelating. They are:
Vitamin C 500-1,000 mg*
Magnesium 400 mg*
Zinc 30-50 mg*
Vitamin E 400IU/day*
Fish Oil (mercury free)
Divided and given 3-4 times per day
Once per day
Some additional recommended supplements are Vitamin A & D, B vitamins (especially mb-12 and methyl folate), Molybdenum & Milk Thistle
Some additional recommended supplements are Vitamin A & D, B vitamins (especially mb-12 and
methyl folate), Molybdenum & Milk Thistle.
Antifungals:
Because eliminating metals can flare yeast, many children also need an antifungal.
There are many natural antifungals to choose from and this page can help you
select the right one for your child.
* this above link is extremely dated! The absolute best anti-fungal to use now in 2025 is the KPV peptide; https://diaryofrecovery.com/kpv
A fear of yeast should not stop you from chelating because metals suppress the
immune system, causing fungal overgrowth in the first place. Yeast also binds to
metals.
Therefore, chelation is something that can end the battle with yeast. Parents often report that near round 50, yeast becomes significantly easier to control.
How do I get started?
I recommend joining the Recovering Kids Facebook Group. There you can ask about
nuances and details specific to certain situations not covered here.
An example is the use of Adrenal Cortex Extract (ACE). Children with low adrenal
function will need to supplement it. I wrote about it here.
You can also buy Andy’s book Amalgam Illness at www.noamalgam.com
Heavy Metal Testing:
I’m inclined to say it’s not critical. It’s also not a requirement for the protocol.
If you have a child with autism and a poor detox system (which goes hand-in-hand)
and that child has been exposed to mercury, what are the chances he or she could benefit from chelation? Very likely — and oftentimes one round will show results.
There are only two tests that will help you determine if you should chelate.
1. Urinary Porphyrin Test – Checks for abnormal levels of porphyrins in the
urine, where different porphyrin levels correlate with body burden of
mercury, lead, or other toxic metals. Performed by a French Lab. We did this test.
2. Hair test – The analysis of this test is tricky and involves “counting rules,” making it
more of an art than a science. There are many children who benefit from chelation
who technically didn’t meet the counting rules. We performed a hair test, but I never
truly figured out if Caroline did or didn’t meet them because it just did not matter
since we were seeing good results from our rounds.
Note: It’s not a good idea to do a challenge test (administering large doses of
chelator and testing urine for metals being excreted). It’s dangerous and proves
nothing. Who wouldn’t excrete large amounts of metals after given high doses of
chelator?

How we Divide the Chelator
1. Open capsule and pour it evenly
into piles in the pill boxes. Stop
when you’ve used about 3/4 of it.
2. Tap the box on its side to determine if they’re equal, use the remaining powder to equalize doses.
If you don’t want to administer to your child via the syringe, you could squirt it back into the cup. We use the syringe which makes it very easy at night.

3. To administer, use a 1 or 3 ml syringe (buy here).
Suction water from a small cup then squirt it into the pill box, stir, and then place the tip in the corner of the box
and suction it back up.
At night, Caroline usually simply swallows and rolls over,
staying asleep.
** TIP: I add melatonin to the midnight dose to help her
stay asleep.
Divided and given
3-4 times per day
Once per day